Cortical Bone Trajectory
The Use of the Bolt® Navigation System to Achieve Precise Cortical Bone Trajectory with Minimal Radiation Exposure
Patient Overview
Age
60
Sex
Male
Diagnosis:
L3-4 stenosis, mild spondylolisthesis and instability


Surgical Treatment
The patient underwent a L3-4 decompression and interbody fusion to relieve pain, stabilize the area, and restore quality of life. The physician elected a posterior Cortical Bone Trajectory (CBT) technique for screw placement due to the many benefits it offers including optimal screw purchase into high-density bone, small incision, less muscle retraction, lower blood loss, shorter surgical time, and directional avoidance of neural anatomy.1 Achieving a precise trajectory is critical in this technique to achieve optimal cortical bone purchase and to prevent a breach of the lateral mass of the vertebral body.
Under surgical treatment, Dr. Thompkins decompressed the compromised anatomy, placed 4 CBT screws using guidance from the Bolt Navigation System, and implanted two TLIF cages at L3-4: a porous titanium TLIF cage and a structural curved allograft.
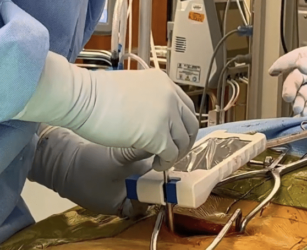

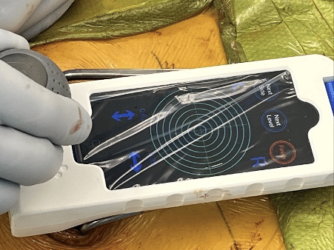
Dr. Thompkins’ technique for cortical screw trajectory with the Bolt Navigation System maximizes accuracy and minimizes radiation exposure.
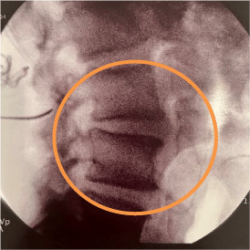
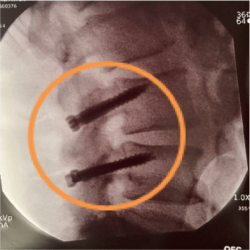
In this approach Caspar pins are placed at the selected entry point for each screw. Once in place a single lateral X-ray and A/P X-ray acquired.
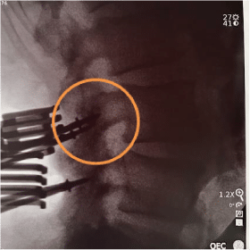
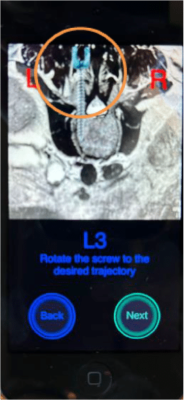
Dr. Thompkins utilizes the pins as reference points to assess each screw’s entry point, angulation, and congruency which allows him to plan any trajectory modifications with the Bolt Navigation System. As an example on the right, Dr. Thompkins corrected the angle of the top right pin while planning and, per the above post-placement X-ray, achieved optimal screw placement.
The use of CBT trajectory requires increased accuracy due to the narrow anatomical placement corridor. In this case, the Bolt Navigation System allowed precise placement of cortical screws with a more confined midline surgical access with a straight-on, slightly cranial and divergent screw angulation away from neural elements. Further, it provided fixation through the medial and lateral portions of the cortex providing advanced bony purchase.
The Bolt Navigation System offers Dr. Thompkins the ability to quickly and easily achieve the benefits of cortical trajectory with minimal radiation exposure.2,3 The System leverages limited intraoperative X-rays and the patient’s existing pre-operative MRI or CT to provide efficient, precise, and low-radiation navigation for this minimally invasive approach.

Outcome
The patient was discharged 3 days after surgery and returned to activity less than 3 months following the procedure.
1 Gutierrez J,Erwood A, Malcom J, Grogan D, Greven A, Gary M, Rodts G, Stricsek G, Refai D Comparing Cortical Bone Trajectory and Traditional Pedicle Screws in Transforaminal Lumbar Interbody Fusion: A retrospective Cohort Study of One-Year Outcomes.Cureus. 2023 Aug; 15(8).
2 Zhang J,Weir V, FajardoL,Lin J, HsiungH, Ritenour ER. Dosimetric characterization of a cone-beam O-arm imaging system. J Xray Sci Technol. 2009;17(4):305-317.
3 Mendelsohn D, Strelzow J, Dea N, et al. Patient and surgeon radiation exposure during spinal instrumentation using intraoperative computed tomography-based navigation. Spine J. 2016;16(3):343-354